


Obligatory - This is not medical advice
You’re going to have to forgive me for these puns.
So, what is an osteosarcoma? It’s a tumor formed of malignant cells that produce bone. This is what we see under the microscope. Amongst disorganized, multiplying, atypical cells (eg the cancer part), we see bone. It’s not an incredibly specific definition, and so it gets deeper. Here’s a picture of what it looks like under the microscope to see a high grade osteosarcoma. I’ve circled an area of osteoid formation.

https://www.pathologyoutlines.com/topic/boneosteosarcomageneral.html
Adding to the complexity, we comment on the ‘grade’ of the tumor, a somewhat inexact measure of how much the cancer cells look like normal tissue and exhibit normal behavior. Within grading, there are low grade tumors that appear very close to normal bone, high grade tumors that are more malignant in character, and intermediate grade tumors that are somewhere in between.
Who gets osteosarcoma?
Osteosarcoma is thought of more so, as a disease of adolescents and young adults. See the below figure from the SEER database.
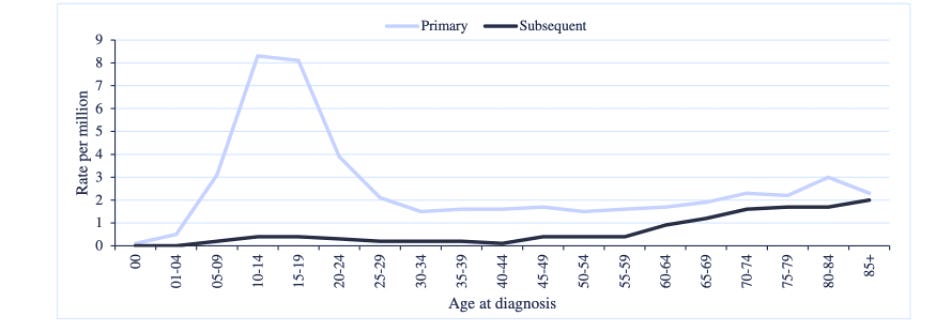
Above is a plot derived from work describing trends in ages of patients with primary and secondary osteosarcoma. 1 The peak incidences occur between the ages of 9 and 24, with a second peak between ages 80 and 84. Looking at this chart, it’s clear to see that this is a cancer of youth. There are numerous risk factors including prior radiation exposure, some hereditary conditions.
So how do we treat it?
As in other parts, you’re going to see me say something along the lines of ‘it depends.’ I can tell you what’s most clearly been shown, but there are inevitably going to lingering uncertainties. Who benefits from what therapy? As we saw above, this is a disease that primarily affects young people. What of those patients who are older than the median of 12? We have some answers, but not all.
What we do know is that for high grade osteosarcoma, chemotherapy improves outcomes. A landmark study for this was published by Link et al. in the New England Journal of Medicine in 1986.2 How did they prove this?
They randomized 36 patients into two groups:
1. Adjuvant chemotherapy
2. No adjuvant chemotherapy
The regimen was very different from that which is given now. Nonetheless, the outcomes were staggering.
33% of patients in the chemotherapy arm had their cancer come back, compared to 83% in the control arm. Even though the numbers were small, the results were significant and have further shaped the treatment of patients with osteosarcoma to this day. Here’s an approximation of that figure.

Not long after, a trial with the following comparison was performed:
1. Doxorubicin and cisplatin given alone
2. Doxorubicin and cisplatin combined with high dose methotrexate.
Here, there was no difference in overall or relapse free survival.3 There is still some controversy regarding the use of methotrexate, and meta-analyses seem to indicate there could be benefit pediatric patients.4
I’m going to leave this post here, but don’t worry, we’ll be revisiting osteosarcoma, treatment, trials, and other data. For now, know that for resectable, high grade disease, chemotherapy is almost always recommended.
https://pubmed.ncbi.nlm.nih.gov/35226758/
https://pubmed-ncbi-nlm-nih-gov.ucsf.idm.oclc.org/3520317/
https://pubmed.ncbi.nlm.nih.gov/1403038/
https://pubmed.ncbi.nlm.nih.gov/21703851/
It makes bone!